Comparison of INSTI vs EFV
STARTMRK Study: raltegravir vs efavirenz,�in combination with TDF/FTC
Original article : Lancet. 2009 Sep 5;374(9692):796-806 - JL Lennox, J Acquir Immune Defic Syndr. 2013 May 1;63(1):77-85 - JK Rockstroh
Last update :
08/10/2014
Dr Anton Pozniak
Chelsea and Westminster Hospital
London, UK

- At 48 weeks of treatment, RAL was non-inferior to EFV, in combination with TDF/FTC. Virologic non-inferiority of RAL was confirmed through W24. RAL was superior to EFV for virologic outcome at week 240
- RAL + TDF/FTC led to more rapid viral load decline (significantly more patients with HIV RNA < 50 c/mL for weeks 2 to 16)
- Greater increase in CD4 was observed in the RAL group. It was significant from W156
- Upon virologic failure, resistance mutations to RAL was found in few cases
- RAL was associated with significantly fewer overall and drug-related clinical adverse events, and CNS-related adverse events than was EFV
- Mean changes in lipid parameters were smaller for RAL than for EFV
- RAL + TDF/FTC is an alternative to EFV + TDF/FTC as a first-line combination regimen in treatment-naïve HIV-infected patients

Design :

*Randomisation was stratified by baseline HIV RNA (< or > 50,000 c/mL) and viral hepatitis co-infection status
Objective :
- Non inferiority of RAL vs EFV: % HIV RNA < 50 c/mL by per protocol, non-completer = failure analysis (lower margin of the 2-sided 95% CI for the difference = - 12%, 90% power)
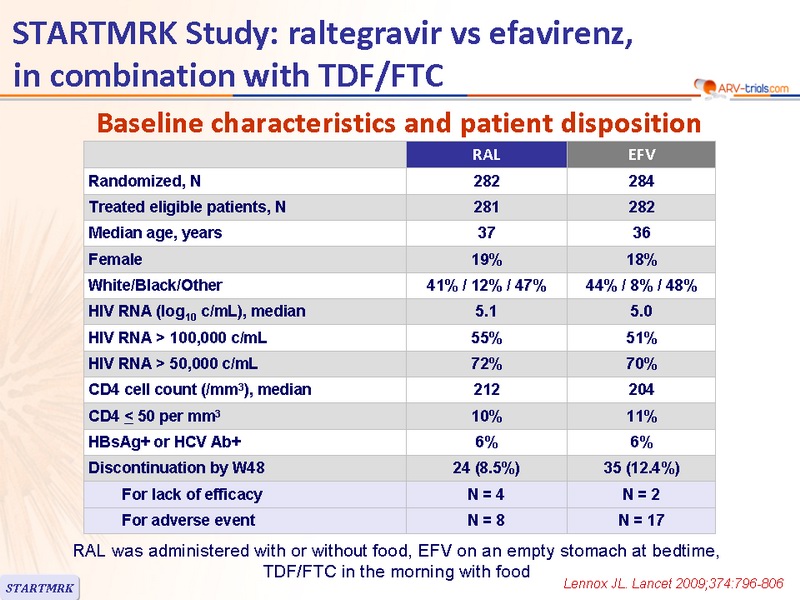
Baseline characteristics and patient disposition :

RAL was administered with or without food, EFV on an empty stomach at bedtime, TDF/FTC in the morning with food
Response to treatment at week 48 :

* Exclusion of discontinuations due to intolerability or reasons unrelated to treatment
Safety at W48 :

Safety: neuropsychiatric symptoms :
- At Week 8
- CNS-related adverse events had occurred in 10% of RAL patients vs 18% of EFV patients (P = 0.0149)
- Retrospective sensitivity analysis (additional symptoms): > 1 CNS-related adverse event: 20% vs 52% (P < 0.0001)
- Most symptoms were self-limited
- At Week 48
- Cumulative incidence of CNS-related adverse event was significantly lower in patients on RAL: 14% vs 23% in the main analysis (P = 0.0044); 26% vs 59% in the sensitivity analysis (P < 0.0001)
- These events were generally mild: 62% of RAL vs 79% of EFV
- Only 1 patient, on EFV, discontinued the trial because of CNS-related adverse event
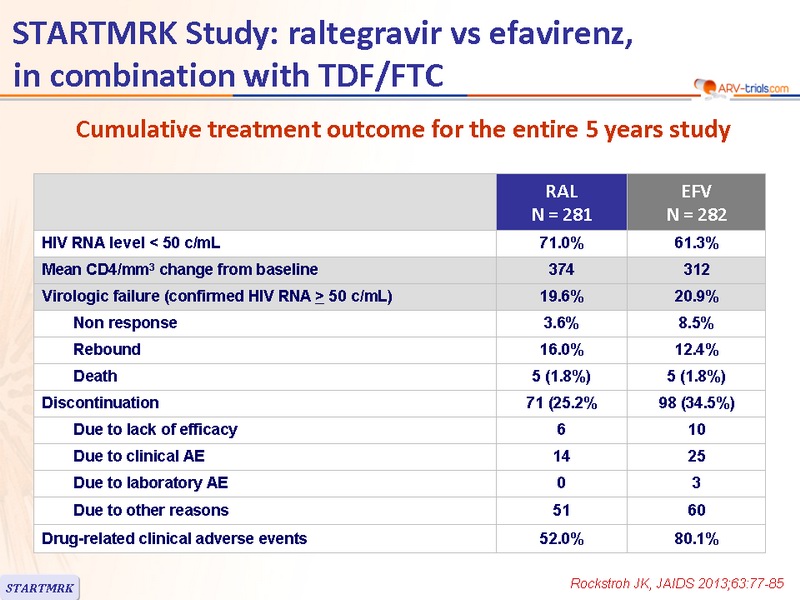
Cumulative treatment outcome for the entire 5 years study :

Cumulative Discontinuation Rate due to AE (%) :

Response to treatment at week 240 (5 years)

Increases in fasting serum triglycerides, total cholesterol, HDL cholesterol, and LDL cholesterol from baseline were significantly lower at W240 (P < 0.005) in RAL than EFV
* Exclusion of discontinuations due to intolerability or reasons unrelated to treatment
Cumulative summary of genotypicresistance data for patients �with RNA > 400 c/mL at the time of virologic failure out to week 240

* Integrase gene could not be amplified in 5 cases
- Emergence of RAL resistance in 4 patients (1.4%)�
Sequencing data of the 4 patients with emergence of RAL-associated mutations
- Q148H + G140S,
- Q148R + G140S,
- Y143Y/H + L74L/M + E92Q +T97A,
- Y143R
Drug-related adverse events in > 5% in either group over 5 years :

 Back to Table of Contents
Back to Table of Contents